


 Sign Out
Sign Out



Pharmacodynamic effects: Paliperidone is a centrally active dopamine Type 2 (D2) receptor antagonist and a serotonin Type 2 (5HT2A) receptor antagonist. Paliperidone is also active as an antagonist at α1 and α2 adrenergic receptors and H1 histaminergic receptors, which may explain some of the other effects of the drug. Paliperidone has no affinity for cholinergic muscarinic or β1- and β2-adrenergic receptors. The pharmacological activity of the (+)- and (-)- paliperidone enantiomers is qualitatively and quantitatively similar in vitro.
Clinical Studies: The efficacy of INVEGA TRINZA for the treatment of schizophrenia in patients who have been adequately treated for at least 4 months with INVEGA SUSTENNA (1-month paliperidone palmitate extended-release injectable suspension) was evaluated in a long-term double-blind, placebo-controlled randomized-withdrawal trial designed to evaluate time to relapse involving adult subjects who met DSM-IV-TR criteria for schizophrenia.
Patients could enter the study with acute symptoms (if previously treated with oral antipsychotics) or be clinically stable (if treated with long-acting injectable antipsychotics [LAI]). All patients who previously received oral antipsychotics received the paliperidone palmitate 1-month initiation regimen (deltoid injections of 150 mg and 100 mg one week apart), while those patients switching from LAI medication were treated with the 1-month paliperidone palmitate extended-release injectable suspension in place of the next scheduled injection. Specifically: For patients entering the study who were already being treated with the 1-month paliperidone palmitate extended-release injectable suspension, their dosing remained unchanged. Patients who were currently receiving the 39 mg dose of 1-month paliperidone palmitate were not eligible to enroll in the study.
Patients entering the study who were being treated with 25 mg, 37.5 mg, or 50 mg of RISPERDAL CONSTA (risperidone long-acting injection) were switched to 50 mg, 75 mg, or 100 mg, respectively, of the 1-month paliperidone palmitate administered in the deltoid muscle.
Patients entering the study who were being treated with any other LAI product were switched to 150 mg of the 1-month paliperidone palmitate administered in the deltoid muscle.
This study consisted of the following three treatment periods: A 17-week flexible-dose open-label period with the 1-month paliperidone palmitate (first part of a 29-week open-label stabilization phase). A total of 506 patients entered this phase of the study. Dosing of the 1-month paliperidone palmitate was individualized based on symptom response, tolerability, and previous medication history. Specifically, the dose could be adjusted at the week 5 and 9 injections and the injection site could be deltoid or gluteal. The week 13 dose had to be the same as the week 9 dose. Patients had to be clinically stable at the end of this period before receiving INVEGA TRINZA at the week 17 visit. Clinical stability was defined as achieving a PANSS total score <70 at week 17. The PANSS is a 30-item scale that measures positive symptoms of schizophrenia (7 items), negative symptoms of schizophrenia (7 items), and general psychopathology (16 items), each rated on a scale of 1 (absent) to 7 (extreme); total PANSS scores range from 30 to 210.
A 12-week open-label treatment period with INVEGA TRINZA (second part of a 29-week open-label stabilization phase). A total of 379 patients received a single-dose of INVEGA TRINZA which was a 3.5 multiple of the last dose of the 1-month paliperidone palmitate. Patients had to remain clinically stable before entry into the next period (double-blind). Clinical stability was defined as achieving a PANSS total score <70 and scores of ≤ 4 for seven specific PANSS items.
A variable length double-blind treatment period. In this period, 305 stabilized patients were randomized 1:1 to continue treatment with INVEGA TRINZA or placebo until relapse, early withdrawal, or the end of study. Patients were randomized to the same dose of INVEGA TRINZA they received during the open-label phase (i.e., 175 mg, 263 mg, 350 mg, or 525 mg) or to placebo administered every 12 weeks. The numbers (%) of patients entering double-blind on each of the dose levels were 6 (4%) for 175 mg, 15 (9%) for 263 mg, 78 (49%) for 350 mg, and 61 (38%) for 525 mg.
The primary efficacy variable was time to first relapse. Relapse was pre-defined as emergence of one or more of the following: psychiatric hospitalization, ≥ 25% increase (if the baseline score was > 40) or a 10-point increase (if the baseline score was ≤ 40) in total PANSS score on two consecutive assessments, deliberate self-injury, violent behavior, suicidal/homicidal ideation, or a score of ≥ 5 (if the maximum baseline score was ≤ 3) or ≥ 6 (if the maximum baseline score was 4) on two consecutive assessments of the specific PANSS items.
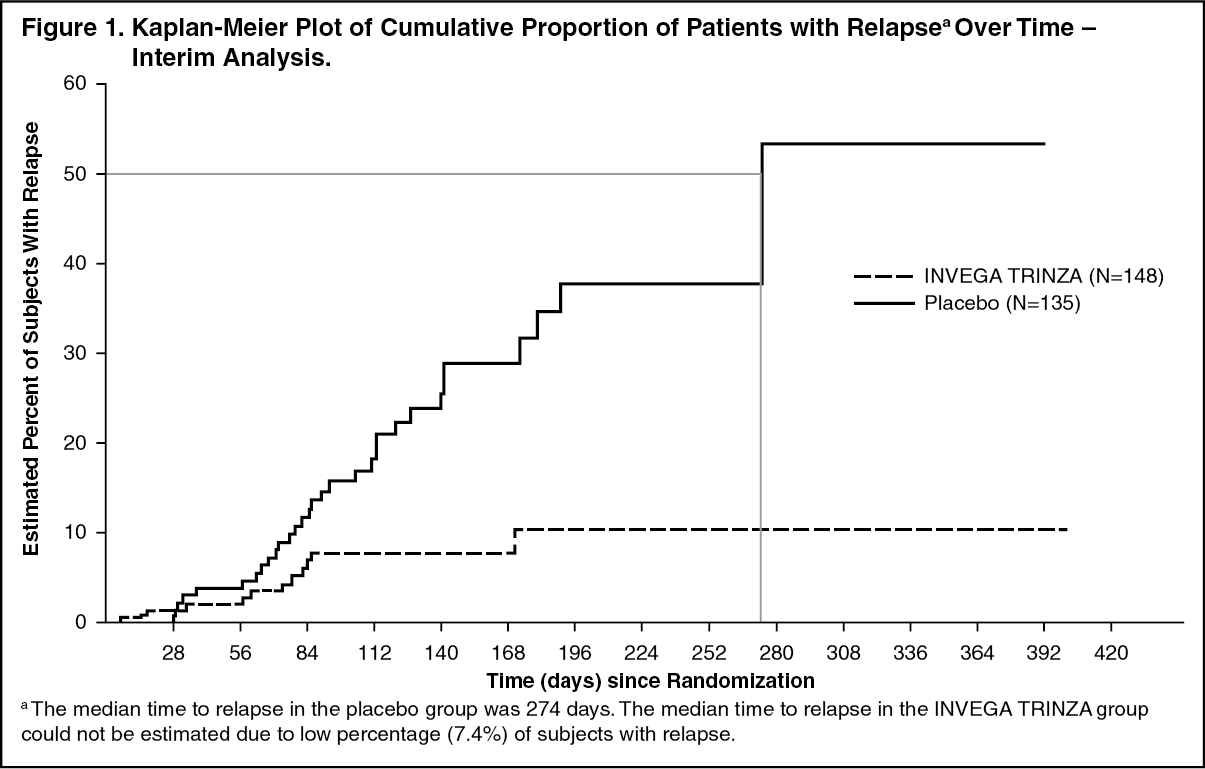
A pre-planned interim analysis showed a statistically significantly longer time to relapse in patients treated with INVEGA TRINZA compared to placebo, and the study was stopped early because efficacy was demonstrated. The most common reason for relapse observed across both treatment groups was increase in the PANSS total score value, followed by psychiatric hospitalization.
Twenty-three percent (23%) of patients in the placebo group and 7.4% of patients in the INVEGA TRINZA group experienced a relapse event. The time to relapse was statistically significantly longer in patients randomized to the INVEGA TRINZA group than compared to placebo-treated patients. A Kaplan-Meier plot of time to relapse by treatment group is shown in Figure 1.
An examination of population subgroups did not reveal any clinically significant differences in responsiveness on the basis of gender, age, or race. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption and Distribution: Due to its extremely low water solubility, the 3-month formulation of paliperidone palmitate dissolves slowly after intramuscular injection before being hydrolyzed to paliperidone and absorbed into the systemic circulation. The release of the drug starts as early as day 1 and lasts for as long as 18 months.
Following a single intramuscular dose of INVEGA TRINZA, the plasma concentrations of paliperidone gradually rise to reach maximum plasma concentrations at a median Tmax of 30-33 days. Following intramuscular injection of INVEGA TRINZA at doses of 175-525 mg paliperidone (as 273-819 mg paliperidone palmitate) in the deltoid muscle, on average, an 11-12% higher Cmax was observed compared with injection in the gluteal muscle. The release profile and dosing regimen of INVEGA TRINZA results in sustained therapeutic concentrations over 3 months. The total and peak exposure of paliperidone following INVEGA TRINZA administration was dose-proportional over a 175-525mg paliperidone (as 273-819 mg paliperidone palmitate) dose range. The mean steady-state peak:trough ratio for a INVEGA TRINZA dose was 1.6 following gluteal administration and 1.7 following deltoid administration. Following administration of INVEGA TRINZA, the apparent volume of distribution of paliperidone is 1960 L.
The plasma protein binding of racemic paliperidone is 74%.
Following administration of INVEGA TRINZA, the (+) and (-) enantiomers of paliperidone interconvert, reaching an AUC (+) to (-) ratio of approximately 1.7-1.8.
Metabolism and Elimination: In a study with oral immediate-release 14C-paliperidone, one week following administration of a single oral dose of 1 mg immediate-release 14C-paliperidone, 59% of the dose was excreted unchanged into urine, indicating that paliperidone is not extensively metabolized in the liver. Approximately 80% of the administered radioactivity was recovered in urine and 11% in the feces. Four metabolic pathways have been identified in vivo, none of which accounted for more than 10% of the dose: dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission. Although in vitro studies suggested a role for CYP2D6 and CYP3A4 in the metabolism of paliperidone, there is no evidence in vivo that these isozymes play a significant role in the metabolism of paliperidone. Population pharmacokinetics analyses indicated no discernible difference on the apparent clearance of paliperidone after administration of oral paliperidone between extensive metabolizers and poor metabolizers of CYP2D6 substrates.
The median apparent half-life of paliperidone following INVEGA TRINZA administration over the dose range of 175-525 mg paliperidone (as 273-819 mg paliperidone palmitate) ranged from 84-95 days following deltoid injections and 118-139 days following gluteal injections. The concentration of paliperidone remaining in the circulation 18 months after dosing of 525 mg paliperidone (as 819 mg paliperidone palmitate) INVEGA TRINZA is stopped is estimated to be 3% (following deltoid injection) or 7% (following gluteal injection) of the average steady-state levels.
Long-acting 3-month paliperidone palmitate injection versus other paliperidone formulations INVEGA TRINZA is designed to deliver paliperidone over a 3-month period, while 1-month paliperidone palmitate injection is administered on a monthly basis. INVEGA TRINZA, when administered at doses that are 3.5-fold higher than the corresponding dose of 1-month paliperidone palmitate injection, results in paliperidone exposures similar to those obtained with corresponding monthly doses of 1-month paliperidone palmitate injection and corresponding once daily doses of paliperidone extended-release tablets. The exposure range for INVEGA TRINZA is encompassed within the exposure range for the approved dose strengths of paliperidone extended-release tablets.
The between-subject variability for paliperidone pharmacokinetics following delivery from INVEGA TRINZA was similar to the variability for paliperidone extended-release tablets. Because of the difference in median pharmacokinetic profiles among the three formulations, caution should be exercised when making a direct comparison of their pharmacokinetic properties.
Drug Interaction Studies: No specific drug interaction studies have been performed with INVEGA TRINZA. The information as follows is obtained from studies with oral paliperidone.
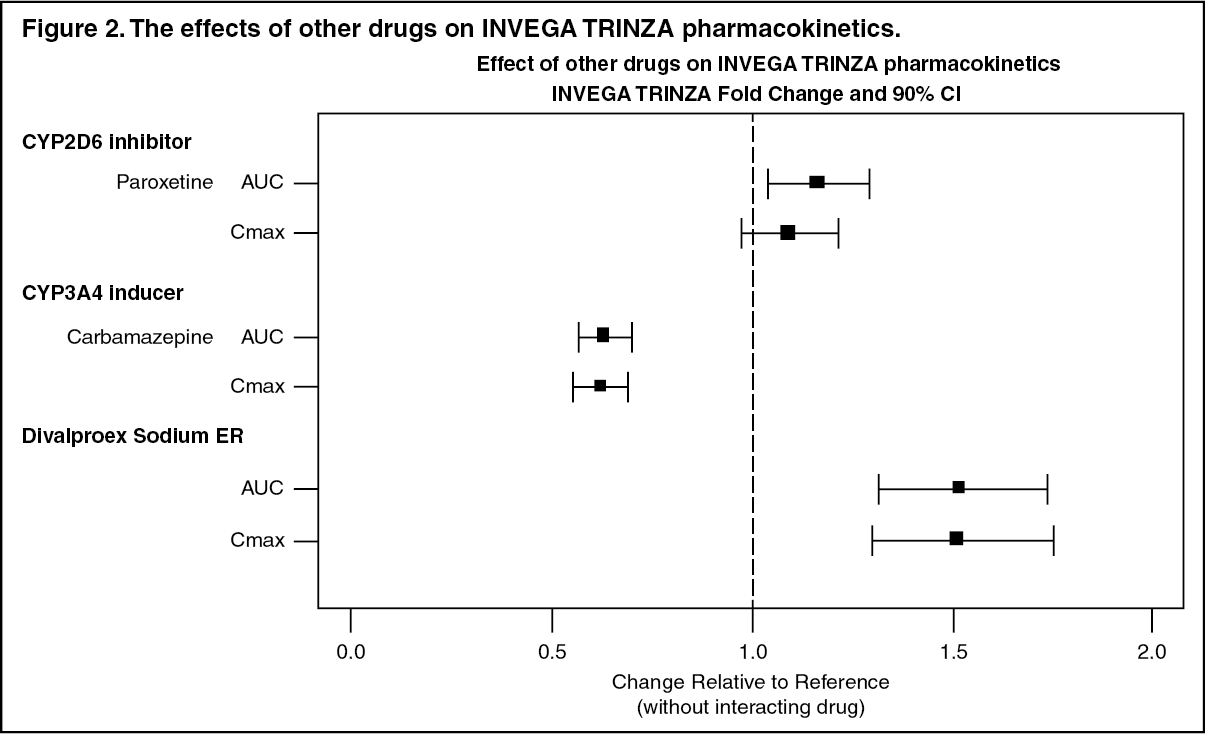
Effects of other drugs on the exposures of INVEGA TRINZA are summarized in Figure 2. After oral administration of 20 mg/day of paroxetine (a potent CYP2D6 inhibitor), an increase in mean Cmax and AUC values at steady-state was observed (see Figure 2). Higher doses of paroxetine have not been studied. The clinical relevance is unknown. After oral administration, a decrease in mean Cmax and AUC values at steady state is expected when patients are treated with carbamazepine, a strong inducer of both CYP3A4 and P-gp (see Drugs Having Clinically Important Interactions with INVEGA TRINZA under Interactions). This decrease is caused, to a substantial degree, by a 35% increase in renal clearance of paliperidone. (See Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn vitro studies indicate that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism, however, there is no evidence in vivo that inhibitors of these enzymes significantly affect the metabolism of paliperidone; they contribute to only a small fraction of total body clearance. In vitro studies demonstrated that paliperidone is a substrate of P-glycoprotein (P-gp) (see Drugs Having No Clinically Important Interactions with INVEGA TRINZA under Interactions).
In vitro studies in human liver microsomes demonstrated that paliperidone does not substantially inhibit the metabolism of drugs metabolized by cytochrome P450 isozymes, including CYP1A2, CYP2A6, CYP2C8/9/10, CYP2D6, CYP2E1, CYP3A4, and CYP3A5. Therefore, paliperidone is not expected to inhibit clearance of drugs that are metabolized by these metabolic pathways in a clinically relevant manner. Paliperidone is also not expected to have enzyme inducing properties.
Paliperidone is a weak inhibitor of P-gp at high concentrations. No in vivo data are available, and the clinical relevance is unknown.
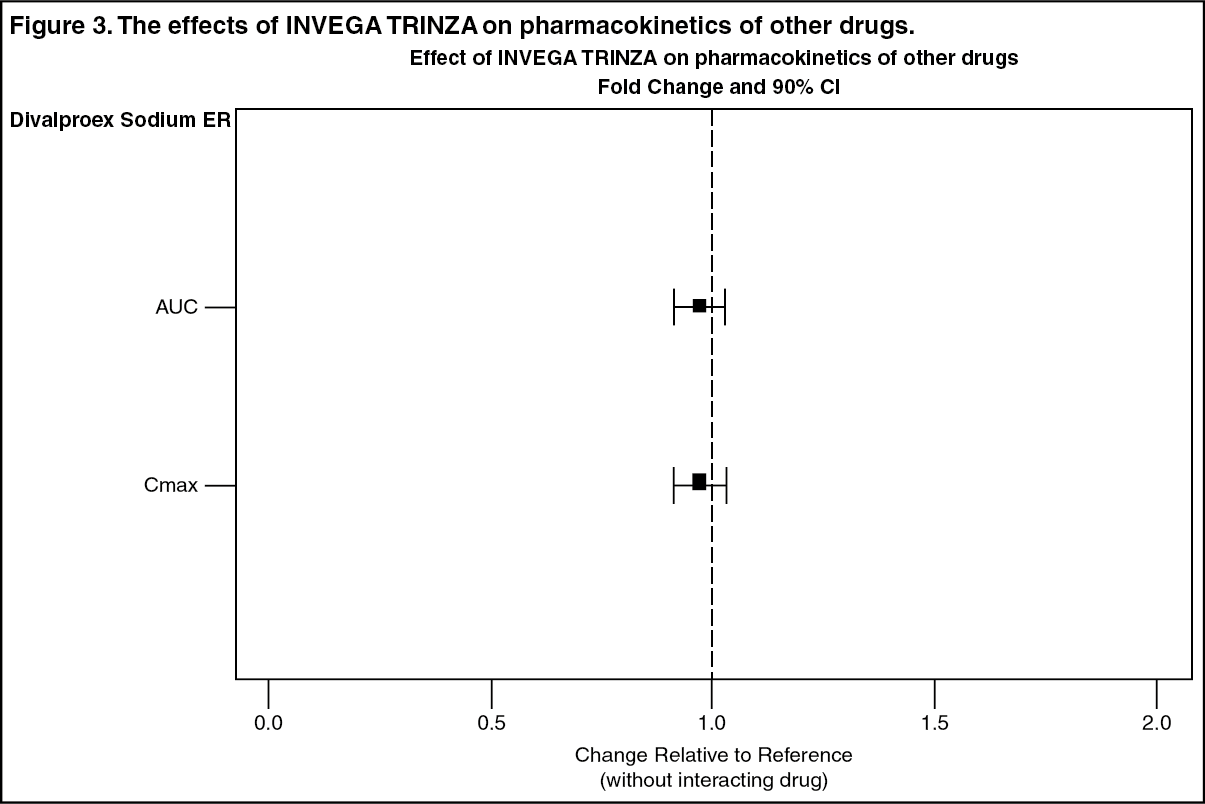
The effects of INVEGA TRINZA on the exposures of other drugs are summarized in Figure 3.
After oral administration of paliperidone, the steady-state Cmax and AUC of valproate were not affected in 13 patients stabilized on valproate. In a clinical study, subjects on stable doses of valproate had comparable valproate average plasma concentrations when oral paliperidone extended-release tablets 3-15 mg/day was added to their existing valproate treatment (see Drugs Having Clinically Important Interactions with INVEGA TRINZA under Interactions). (See Figure 3.)
 Click on icon to see table/diagram/image
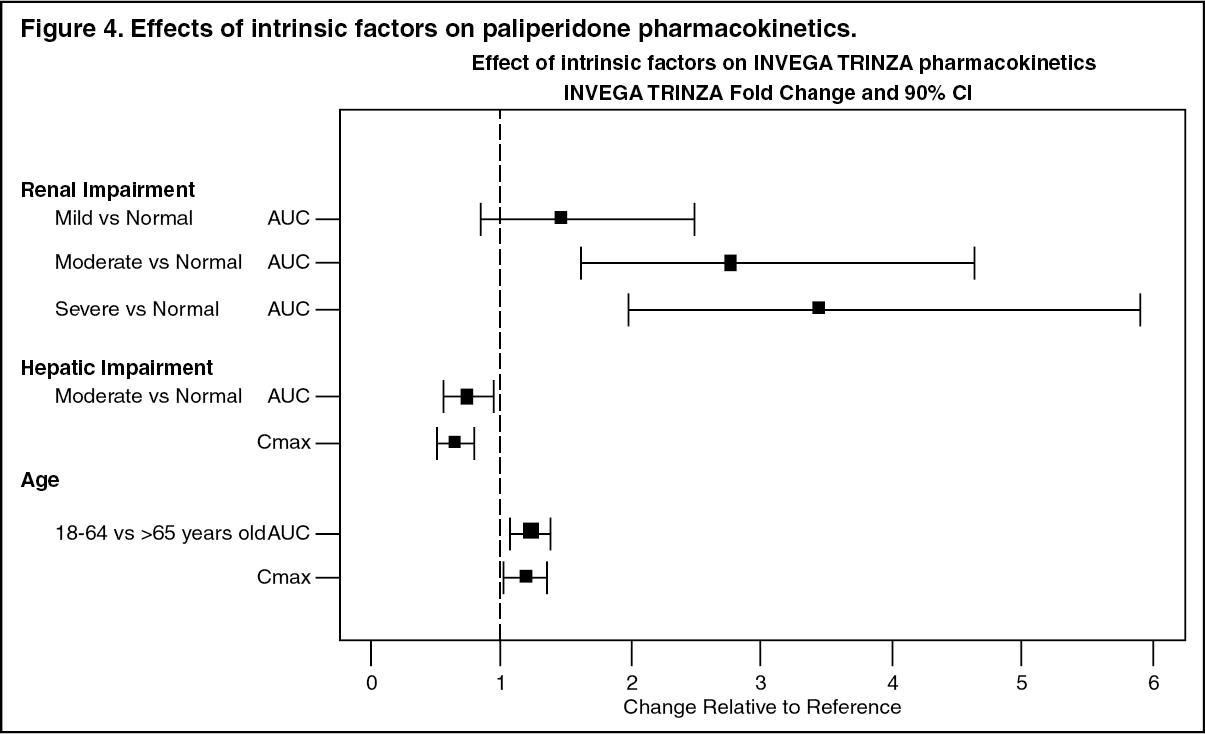
Click on icon to see table/diagram/imageStudies in Specific Populations: No specific pharmacokinetic studies have been performed with INVEGA TRINZA in specific populations. All the information is obtained from studies with oral paliperidone or is based on the population pharmacokinetic modelling of oral paliperidone and INVEGA TRINZA. Exposures of paliperidone in specific populations (renal impairment, hepatic impairment and elderly) are summarized in Figure 4 (see Dosage Adjustment in Renal Impairment under Dosage & Administration and Use in Specific Populations: Renal Impairment under Precautions).
After oral administration of paliperidone in patients with moderate hepatic impairment, the plasma concentrations of free paliperidone were similar to those of healthy subjects, although total paliperidone exposure decreased because of a decrease in protein binding. Paliperidone has not been studied in patients with severe hepatic impairment (see Use in Specific Populations: Hepatic Impairment under Precautions).
After oral administration of paliperidone in elderly subjects, the Cmax and AUC increased 1.2-fold compared to young subjects. However, there may be age-related decreases in creatinine clearance (see Dosage Adjustment in Renal Impairment under Dosage & Administration and Use in Specific Populations: Use in Elderly under Precautions). (See Figure 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBased on in vitro studies utilizing human liver enzymes, paliperidone is not a substrate for CYP1A2; smoking should, therefore, not have an effect on the pharmacokinetics of paliperidone. Slower absorption was observed in females in a population pharmacokinetic analysis. At apparent steady-state with INVEGA TRINZA, the trough concentrations were similar between males and females.
Lower Cmax was observed in overweight and obese subjects. At apparent steady-state with INVEGA TRINZA, the trough concentrations were similar among normal, overweight, and obese subjects.
Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis: No carcinogenicity studies were conducted with the 3-month paliperidone palmitate extended-release injectable suspension.
The carcinogenic potential of intramuscular injection of 1-month paliperidone palmitate extended-release injectable suspension was assessed in rats. There was an increase in mammary gland adenocarcinomas in female rats at 16, 47, and 94 mg/kg/month, which are 0.2, 0.6 and 1 times the maximum recommended human dose (MRHD) of 525 mg paliperidone (as 819 mg paliperidone palmitate) of 3-month paliperidone palmitate extended-release injectable suspension on mg/m2 basis. A no-effect dose was not established. Male rats showed an increase in mammary gland adenomas, fibroadenomas, and carcinomas at doses, which are 0.6 and 1 times the MRHD of 525 mg paliperidone (as 819 mg paliperidone palmitate) of 3-month paliperidone palmitate extended-release injectable suspension on mg/m2 basis. A carcinogenicity study in mice has not been conducted with the 1-month paliperidone palmitate extended-release injectable suspension.
Carcinogenicity studies of risperidone, which is extensively converted to paliperidone in rats, mice, and humans, were conducted in Swiss albino mice and Wistar rats. Risperidone was administered in the diet for 18 months to mice and for 25 months to rats at daily doses of 0.63, 2.5, and 10 mg/kg/day, which are 0.2 to 3 times in mice and 0.4 to 6 times in rats the MRHD of 16 mg/day of risperidone on mg/m2 basis. A maximum tolerated dose was not achieved in male mice. There were statistically significant increases in pituitary gland adenomas, endocrine pancreas adenomas, and mammary gland adenocarcinomas. The no-effect dose for these tumors was less than or equal to the MRHD of risperidone on mg/m2 basis (see RISPERDAL package insert). An increase in mammary, pituitary, and endocrine pancreas neoplasms has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be mediated by prolonged dopamine D2-receptor antagonism and hyperprolactinemia. The relevance of these tumor findings in rodents in terms of human risk is unknown (see Hyperprolactinemia under Precautions).
Mutagenesis: No mutagenesis studies were conducted with the 3-month paliperidone palmitate extended-release injectable suspension.
Paliperidone palmitate showed no genotoxicity in the in vitro Ames bacterial reverse mutation test and mouse lymphoma assay. Paliperidone was not genotoxic in the in vitro Ames bacterial reverse mutation test, mouse lymphoma assay and the in vivo rat bone marrow micronucleus test.
Impairment of Fertility: No fertility studies were conducted with the 3-month paliperidone palmitate extended-release injectable suspension.
In a rat fertility study orally administered paliperidone increased pre- and post-implantation losses and slightly decreased the number of live embryos at doses up to 2.5 mg/kg/day, a dose which is 2 times the MRHD of 12 mg on mg/m2 basis. This dose also caused slight maternal toxicity but there was no effect on the percentage of treated female rats that became pregnant. Pre- and post-implantation losses, the number of live embryos and maternal toxicity were not affected at 0.63 mg/kg/day, a dose, which is half of the MRHD of 12 mg/day of orally administered paliperidone on mg/m2 basis. The fertility of male rats was not affected at oral doses of paliperidone of up to 2.5 mg/kg/day, which are up to 2 times the MRHD of 12 mg on mg/m2 basis, although sperm count and sperm viability studies were not conducted with paliperidone.
In a sub-chronic study in Beagle dogs with risperidone, which is extensively converted to paliperidone in dogs and humans, all doses tested 0.31 to 5.0 mg/kg/day, which are 0.6 to 10 times the MRHD of 16 mg on mg/m2 basis, resulted in decreases in serum testosterone and decreases in sperm motility and concentration. Serum testosterone and sperm parameters partially recovered, but remained decreased at the last observation two months after treatment was discontinued.
Animal Toxicology and/or Pharmacology: Injection site toxicity was assessed in minipigs injected intramuscularly with the 3-month paliperidone palmitate extended-release injectable suspension at doses up to 525mg paliperidone (as 819 mg paliperidone palmitate), which is equal to the MRHD. Injection site inflammatory reactions were greater and more advanced than reactions to the 1-month paliperidone palmitate extended-release injectable suspension. Reversibility of these findings was not examined.